March 16, 1998
The health care industry is in a constant state of change. In the past, the traditional practice for reimbursement was on a fee-for-service basis. Those days are numbered. The new environment is shifting towards capitation or a fixed rate for each covered life. The focus of health care providers will be to provide quality care at the lowest possible cost. To compete on the basis of quality, the information integrity is paramount. To accomplish this feat, it is imperative to have access to information that is valid, timely, rapidly accessed and convenient to attain. Automation of the operating room is critical to ascertain patterns, assist in problem solving, manage productivity and resources, and provide data to support sound management decisions.
Surgical services impact on more than fifty percent of the economic performance of a hospital. Hospital executives view the operating room as a major cost center, but few view it as a principal profit center. An efficiently run operating room with definable revenues and costs can prove to be an invaluable asset to the entire organization.
Eighty-five percent of the U.S. operating rooms have some type of information system, but it is the rare exception of one that is fully integrated throughout its perioperative system.
The efficient scheduling of surgical procedures in the operating room suites is dependent on maximizing the use of each suite, while accommodating the surgeons' requests for a specific date, time, routine supplies, and any special instruments and/or supplies required for the procedure. Tracking surgeons' preferences and average times for procedures is cumbersome and often inaccurate without the benefit of computerization, especially in an environment having many surgeons and a high volume of procedures.
Without easily accessible and accurate historical information for average times, delays in the schedule will impact negatively on customer service and drive costs upward. If information is difficult to attain, cost analysis per procedure or economic credentialing for individual surgeons proves to be almost impossible to attain.
The operating room impacts the clinical, financial, and administrative practices of many other departments throughout the hospital. From the time the procedure is scheduled, until the patient is discharged, accurate information must be communicated to ensure that efficient and effective patient care is provided as well as the proper allocation of resources.
The selection and the designing of a HMIS system appropriate for the needs of the perioperative service will prove to enhance the ability to gather, update and maintain a shared database. With this ability, information handling will become more efficient, timely, and cost effective. Some proven benefits would include: a) reduced operational costs by better allocation of human resources, b) reduced inventories, c) reduced delays, d) increased revenues, e) increased customer satisfaction, f) increased employee satisfaction, and g) timely information to support decision-making.
There are many factors that must be taken into account prior to the implementation of a new HMIS. With any change, the culture of the organization must be assessed. This assessment must include the organization's strategic goals, beliefs, and the varied management styles of the individuals that work within the organization. Successful implementation cannot be accomplished if the culture does not foster commitment to the change. In order to manage the change that will come with implementing the HMIS, there must be a clear plan, skills assessed, resources supplied, incentives offered and illustrated, and the provision of customer support.
The information system must incorporate the strategic plan of the organization. It is imperative that it supports the business processes that are required in making decisions, accommodates the daily activities, and assists in the management of its resources.
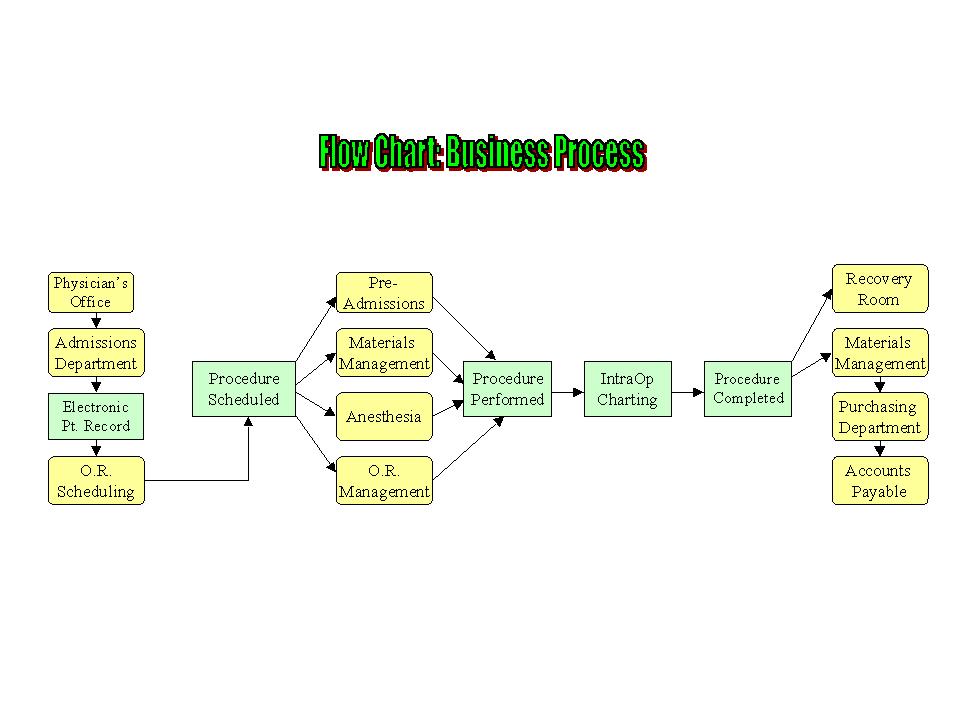
One of the first steps in planning the implementation of a HMIS is to look at the business processes and identify what will be required of that information system to facilitate the daily operations of the organization. It would then be beneficial to identify the major customers and/or players that will be interacting with the system. They are listed below somewhat in the order of which they enter the system. (See the following flowchart).
The process begins when the physician requests a procedure to be posted. In most situations, the procedure is not an emergency or urgent in nature and is scheduled some time in the future. This is referred to as an elective procedure. The call is usually placed by the surgeon's clerical staff to the Admissions department. The Admissions department is the first to receive patient information. The ideal HMIS will make this information available to the surgical information system through an interface.
Once the patient's demographic information and insurance coverage is clarified, the next players to enter the system are the operating room schedulers. The schedulers input information for the specific procedure, surgeon, and date requested. A user-defined procedure code is then entered. The system determines a case length by averaging the last ten times that procedure code was assigned to that surgeon in determining the length of time necessary. Utilizing computerized historical data is optimal to maximize the utilization of the operating room suites.
There are usually assigned blocks of times that are built into the system by the end user to facilitate the scheduling of cases. This block time can be service specific, (e.g., Orthopedics), or by individual surgeons on determined days of the week and in specific operating room suites. The surgical information system must allow customization for the practice of an individual operating room. The schedulers must be able to look at the scheduling grid and identify the appropriate operating room suites assigned to the block time.
A key component for maximizing utilization of the operating room schedule is the interaction between the physicians' office staff and the operating room scheduling staff. Education must be offered to the office staff including the provision of a list of procedure codes, scheduling policies, and access to block time assigned to them. The ideal HMIS integrates the physician's office to the scheduling system through a network environment. It enables them to "request" the scheduling of cases in their block time. Once it is requested, the schedulers can confirm whether the case has been officially posted. This option is a time saver for the operating room schedulers and the office staff by eliminating telephone calls, thereby creating a shared responsibility for accurate posting of procedures and improving customer satisfaction.
Notification of conflicts by the system is crucial in managing the resources in the operating room, to minimize delays in procedures. An example of a conflict would be for instrumentation or equipment. The system should allow the input of information into tables linked to specific procedures to identify when a shared resource is overbooked to avoid scrambling the day of surgery for unavailable instruments/equipment used in other suites.
The information in the system must now be shared with the multidisciplinary team in preparation for the scheduled surgeries. The Pre-Admissions department is notified of the pending schedule of cases. They must assure that the patients are medically prepared. This includes gathering information regarding past medical history, as well as laboratory and other tests required by the institution. The anesthesia department is also involved in the preoperative planning of patient care. They utilize the information to determine the type of anesthesia required, any further tests that may be needed, and the anesthesia personnel needed on the day of surgery. The operating room management oversees the schedule to plan for staffing of nursing personnel, equipment, instruments and supplies needed.
It is desirable that the HMIS integrates the information of the scheduling system with the materials management department. The procedure codes selected must generate supply requisitions that are both procedure- and surgeon-specific. These requisitions should have bin locations assigned for each supply item to allow the efficient selection of the items to stock casecarts. The system should then allow the return of any items not used the day of surgery and the subsequent deprecation of items charged to the patient in order to maintain a perpetual inventory.
On the day of surgery, it is necessary to be able to observe the patient flow throughout their perioperative experience. From the time the patients enter the hospital, until they are discharged, they system should provide a tracking system. At a glance, anesthesia and nursing management should be able to know if the patient is ready to be taken into surgery, at what point they are in the procedure, and when they arrive and leave the recovery room. This can be accomplished with a system that allows "real time" charting and integrates this information into a graphic monitoring system. The pre-admission department enters information into the system when the patient is ready for transport to the operating room. The nursing staff in the operating room documents on the computerized patient record when the patient enters the suite, incision time, closure time, and when the patient is transferred to the recovery room. The recovery room can then use the system to input information regarding their stay and subsequent discharge. The capability to track the patient throughout the perioperative stay would facilitate any adjustments needed to keep the schedule running efficiently.
Postoperatively, the information can be used by many different factions in a variety of ways. Computerization of the materials management system is essential to control inventory costs and monitor supply usage. Information gathered will facilitate controlling supply expenses per procedure and eliciting support from physicians in standardization of products. Materials management manages its inventory with the data entered regarding supply usage. An integrated system forecasts needed supplies based on scheduled cases. This information minimizes the required inventory levels. Reports, such as stock status reports, could provide a record of supplies remaining on the shelf and therefore generate requisitions to replenish supplies. With accurate information, the materials management system will help reduce on-hand quantities, increase inventory turns, and work towards a just-in-time system.
The purchasing department should also be integrated with the information system to improve effciency of requisitioning supplies. A requisition is composed and sent to the purchasing department from materials management requesting supplies via the HMIS. It then can utilize EDI to generate purchase orders and interface with major vendors. The last part of the cycle involves integration of the accounts payable department. An integrated system facilitates invoice reconciliation and payment for requisitioned supplies.
The information documented in the computerized patient record affords a wealth of information to support management decisions. The software should contain easy tools to assist management with analysis and improve their effectiveness. Reports supplied by the software and the ability to create ad hoc reports should allow the data to be manipulated in an effort to forecast case loads, track delays in the schedule, analyze costs per procedure and performance by individual surgeons, evaluate the effects of cancellations, and a myriad of other factors that impact on daily operations and demonstrate cost effectiveness.
After identifying the people involved, the business processes, and the data the system should to be able to process, the technical architecture must be determined to accomplish all of the above. A network environment is therefore necessary to collect and distribute data to all individuals required to make the business process work efficiently with the established data architecture. In the not so distant future, web technology could also play an intricate part in the sharing of information. The vendor of choice should provide information regarding PC and other hardware requirements. The IS department should also become very involved with implementation of the plan for the technical architecture.
The last piece to the puzzle is the institution of a control structure. This structure will help to establish policies, standards, and protocols. Assessment of end users' skills and resources should be provided to assure the system is utilized properly. Security levels should be established and enforced by the systems administrator. During orientation of the end users, matters of confidentiality must be stressed and expectations established.
A control structure will assist in looking at the big picture. Sometimes it may be necessary to sacrifice the best individual choice of software to what is good for the whole. Rather than each department selecting a different vendor and opting to interface with the departments that need to share the information, it may be more prudent to opt for an integrated system. This will afford the use of a shared database, reduce redundancy and data anomalies, and therefore prove to be more reliable.
The expectations of the users of the HMIS should be realistic. The HMIS should not be viewed as an answer to all of the problems of the organization. It should be seen as a vehicle in assisting management to make decisions based on facts.
An internet search was performed to identify potential software providers of surgical information systems. Our selection criteria were based on systems that were integrated with the critical departments that would interact with the daily operations of the operating room. The four systems we evaluated are the following:
Advanced Medical Systems (AMS) is a division of Leeward Software, Inc., a leading software development firm specializing in Materials Management Information Systems for the healthcare industry. AMS was founded in 1982 and serves more than 200 healthcare facilities in North America. AMS is based in West Trenton, New Jersey. Their software product, ConTrol, is a real-time comprehensive materials management/operating room management software system.
Advanced Medical Systems' ConTrol system organizes and integrates the entire supply function. All activity, from purchase requisitioning through patient expensing, is brought together, with transactions instantly and simultaneously reflected throughout the system. ConTrol was designed and developed in a multi-entity hospital and continues to excel in multi-facility functionality to monitor the movement of inventory from one hospital to departments or cost centers in other hospitals.
The ConTrol Operating Room module provides the functionality to accurately maintain a surgical case schedule. Operating Room personnel have the capability to modify, record, and monitor all relevant surgical case information. ConTrol provides the means to avoid scheduling conflicts to allow for the efficient management of resources.
The ConTrol Operating Room module is one of several available modules which, as an aggregate, function as an integrated information system. Materials Management, Accounts Payable, Asset Management, Budget Management, and Electronic Data Interchange (EDI) comprise the other available modules.
Founded in 1981, Enterprise Systems, Inc. (ESi), develops, markets, installs and services an integrated suite of application software products that assist healthcare providers in managing their operations. With more than 1,000 clients, ESi pioneered stockless inventory and paperless Electronic Data Interchange (EDI) with over 100 vendors. ESi was acquired by HBO & Company (HBOC) in June of 1997. HBOC, founded in 1974, has grown to become one of the major providers in the healthcare informatics industry and serves the healthcare information systems needs of the health enterprise-hospitals, integrated delivery networks and managed care organizations. HBOC has a customer base of approximately 5,000 community hospitals, 3,800 physician practices, 600 homecare agencies and 600 payors. ESi's corporate headquarters are based in Wheeling, Illinois.
ESi's ORBIT Surgical Services Management module is rich in functionality to provide for the appropriate utilization of operating room resources.
Enterprise Systems, Inc. (ESi) provides an integrated system, consisting of modules for Surgical Services Management, Materials Management, Accounts Payable, Enterprise Scheduling, and Resource Management.
Surgical Information Systems (SIS) was organized in 1993 as a private division of a public healthcare company to deliver software to the hospital or ambulatory surgical department. SIS began operation in 1997 initially as an anesthesiology record keeping system and expanded its features to include surgical department scheduling. SIS corporate offices are in Atlanta, and the product is installed in three sites.
SIS computer applications enable a surgical department to accurately schedule procedures, fully document the intraoperative and postoperative episode, and enable the department manager to accurately assess cost components and cost tracking for the totality of the surgical procedure. In addition, SIS provides an added value through surgical pathways and clinical outcome evaluations. The SIS system captures all clinical, financial, administrative, and archival data needed to manage surgical services and comply with JCAHO quality monitoring requirements.
Serving Software introduced Surgi-Server in 1984 and was acquired by HBO & Company (HBOC) in September, 1994. The Serving Software Group, as a business unit of HBOC, is focused exclusively on building scheduling and resource management solutions for the healthcare industry and is based in Minneapolis. HBOC's Pathways Surgical Manager is an enterprisewide scheduling and resource management solution presently in development which will represent the integration of ESi and Serving Software business units, to produce a single product provided for this market segment by HBOC.
HBOC's Serving Software Group's Surgi-Server is the leading operating room scheduling and management system. Surgi-Server manages case scheduling, charging, charting, staff scheduling, and reporting.
Each Surgi-Server system is personalized, allowing users to define screens, data elements, screen flow, abbreviations, and data flow.
The Surgi-Server Surgical Scheduling module is flexible and can be complemented by the addition of the following modules: Dynamic Scheduling, IntraOperative, Multi-Entity, Surgical Personnel, and Surgical Supply. An Accounts Payable module, however, is not available as a component of an integrated system, although other vendor's products can be interfaced to Surgi-Server.
|
Criteria |
ConTrol |
ESi |
Surgical Info Sys |
Surgi-Server |
|
User Friendliness |
||||
Help command |
Yes |
Yes |
No |
Yes |
Graphical User Interface (GUI) |
Yes |
Yes |
Yes |
No |
|
Surgical Scheduling |
||||
Enterprise-wide scheduling |
No |
Yes |
No |
No |
Block scheduling |
Yes |
Yes |
Yes |
Yes |
Open scheduling |
Yes |
Yes |
Yes |
Yes |
Conflict checking |
Yes |
Yes |
Yes |
Yes |
Preference cards for supplies |
Yes |
Yes |
Yes |
Yes |
Patient charging for inventory usage |
Yes |
Yes |
Yes |
Yes |
Implantable device log |
Yes |
Yes |
Yes |
Yes |
|
Materials Management |
||||
Bar coding capability |
Yes |
Yes |
Yes |
No |
EDI |
Yes |
Yes |
No |
No |
Exchange cart management |
Yes |
Yes |
Yes |
No |
Multiple inventory locations |
Yes |
Yes |
No |
Yes |
Non-stock requisitioning |
Yes |
Yes |
Yes |
Yes |
Pick-list/bin location generation |
Yes |
Yes |
Yes |
Yes |
|
Other System Functionality |
||||
Dynamic day manager |
No |
Yes |
Yes |
Yes |
Physician credentialing |
No |
Yes |
Yes |
Yes |
Pre-operative nursing data |
Yes |
No |
Yes |
No |
Visual instrument catalogue |
No |
Yes |
No |
No |
Remote physician link/access |
No |
Yes |
Yes |
No |
Autofax capability |
No |
Yes |
No |
No |
|
Reports |
||||
Case listings by date |
Yes |
Yes |
Yes |
Yes |
Case listings by operating room |
Yes |
Yes |
Yes |
Yes |
Case listings by surgeon |
Yes |
Yes |
Yes |
Yes |
Delays by cause |
Yes |
Yes |
Yes |
Yes |
Inventory by case |
Yes |
Yes |
Yes |
Yes |
Inventory by procedure |
Yes |
Yes |
Yes |
Yes |
Inventory by surgeon/economic credentialing |
Yes |
Yes |
Yes |
Yes |
Utilization |
Yes |
Yes |
Yes |
Yes |
Ad hoc reporting capability |
No |
Yes |
Yes |
Yes |
|
Data Management |
||||
Security/access levels |
Yes |
Yes |
Yes |
Yes |
Simultaneous access by multiple users |
Yes |
Yes |
Yes |
Yes |
Archiving |
Yes |
Yes |
Yes |
Yes |
|
Vendor Support |
||||
Technical support |
24/7 |
24/7 |
24/7 |
24/7 |
Training program/resources available |
Yes |
Yes |
Yes |
Yes |
|
Hardware & Operating System |
||||
Pc-based network/client-server |
Yes |
Yes |
Yes |
Yes |
Windows environment |
Yes |
Yes |
Yes |
Yes |
HL-7 compliance |
Yes |
Yes |
Yes |
Yes |
Year 2000 compliance |
Yes |
Yes |
Yes |
Yes |
|
Integration/Interfacing |
||||
ADT interface |
Yes |
Yes |
Yes |
Yes |
Accounts Payable - integrated |
Yes |
Yes |
No |
No |
Materials Management - integrated |
Yes |
Yes |
No |
Yes |
Common database |
Yes |
Yes |
No |
No |
|
Cost Factors |
||||
Software cost |
$150,000 |
$200,000 |
$350,000 |
$150,000 |
Annual support cost |
10% |
18% |
12% |
10% |
|
Vendor Profile |
||||
Year product first introduced |
1982 |
1981 |
1997 |
1984 |
Number of installed sites |
200+ |
370 |
3 |
600+ |
Hospital A is utilizing a surgical information system, Surgi-Server. Unfortunately it is eight years old, three versions behind the latest available, and does not "talk" to the ESi system, currently used by materials management, purchasing, and accounts payable. The information that has been entered into the Surgi-Server system is unreliable. Reasons for this includes: a) the supply file has no valid vendor information, price information, or stock levels, b) the patient information file has duplicate data, c) the procedure module has inaccurate codes and unreliable case times assigned to individual surgeons, d) a majority of the user-defined and advanced-user-defined reports (created by the end users) are questionable and number in the thousands, e) Surgi-Server is a DOS- based program that is no longer enhanced, f) some of the modules are obsolete and no longer supported by the vendor, and g) the version being used is not Year 2000 compliant.
A new systems administrator was hired last year to "fix" the system. Since there was no cost associated with upgrading, the organization chose to upgrade rather than invest the capital to reimplement the system. The systems administrator assessed the problems and concluded that it would be more prudent to scrap the current system and install the operating room module provided by ESi.
Both Surgi-Server and ESi are now owned by HBOC. Both are DOS-based and are being phased out. HBOC is developing a new window-based application software called Surgery Manager, which will replace the ESi and Surgi-Server products.
The debate continues and a variety of options have been provided for consideration. They are as follows:
Our recommendation is Option #3, install ESi's operating room module (ORBIT). Since the version of Surgi-Server is not Year 2000 compliant, a change must be instituted in the very near future. Argument would have it that upgrading would be the most cost effective at this point in time and one should wait until the new product is available. The new product is based 90% on the ORBIT module and therefore will be easily migrated to once it is available. Meanwhile, Hospital A can have the convenience of an integrated system.
Hospital B represents any hospital which presently does not have a surgical information system. Manual processes are used for scheduling surgical cases, tracking supplies, materials, and equipment. This leads to inefficiency and dissatisfaction of the stakeholders in the process. Physicians are not as easily accommodated with their scheduling requests. Valuable operating room suites may be under- or over-utilized to insure that a physician's request is honored. It is difficult to maintain adequate inventory since level requirements are based on intuition more than fact. Without automation, staff scheduling may not meet the need of varying volumes of the operating room schedule. Inefficient management of human resources may lead to under-staffing during peak caseloads resulting in overtime or over-staffing during low operating room utilization. Evaluation of the surgical information systems, in this vignette, can be less restrictive than the scenario presented in Vignette 1, since there is no existing system to influence the decision.
Overall, we recommend ESi as the vendor/system of choice. ESi and ConTrol are the only product lines fully integrated throughout modules for operating room management, accounts payable, and materials management. The ideal information system solution for the operating room environment includes a fully integrated system, with a common database that each module shares. Less maintenance is required and there is a greater chance of insuring data integrity, while eliminating redundancies and anomalies. Surgical Information Systems and Surgi-Server do not have fully integrated system solutions and therefore were eliminated from further evaluation.
Functionality among all of the systems evaluated was robust and, with few exceptions, would satisfy the needs of most users. An individual hospital would have to specifically evaluate any of the criteria that may be particularly important to their operations. ESi is the only vendor that offers Autofax capability allowing automatic transmittion of the operating room schedule to preselected sites. Another feature offered by ESi , physician link, allows remote access from the physician's office to request the scheduling of cases in their block time. ESi and SIS are the vendors that offer this function. ESi and ConTrol offer electronic data interchange (EDI) capabilities, whereas SIS and Surgi-Server do not.
The vendor's resources and client base are important criteria for evaluation. We were concerned that Surgical Information Systems was first introduced in 1997 and had only three (installed) sites. ConTrol, ESi, and Surgi-Server are all well-established products which have been refined many times since their initial introduction. HBOC is the vendor for both ESi and Surgi-Server. As one of the market leading vendors of healthcare information systems, HBOC is the only one to provide enterprise-wide solutions to information problems. Enterprise-wide scheduling, for example, is available only through ESi, and coordinates with other clinical departments, such as scheduling a CAT scan.
At this stage, it is difficult to evaluate the systems based on cost. Costs quoted by the vendors is only to be used as a guide, while final pricing is typically negotiated between the vendor and the client.
Bross B, & Gamblin BB, Using a computerized scheduling system to predict procedure lengths. AORN J June 1995; 61(6): 1054-60, 1059-61.
Dexter F, Application of prediction levels to operating room scheduling. AORN J 1996; 63:607-15.
Dexter F, & Macario A, Applications of Information Systems to Operating Room Scheduling. Anesthesiology December 1996; 85(6): 1232-4.
Hamilton DM, & Breslawski, S, Operating room scheduling: Factors to consider. AORN J 1994; 59:665-8, 671-80.
Hancock WM, Walter PF, More RA, & Glick ND, Operating Room Scheduling Data Base Analysis for Scheduling. Journal of Medical Systems 1998; 12(6):397-409.
Kanich, DG, & Byrd JR, How to Increase Efficiency in the Operating Room. Surgical Clinics of North America February 1996; 76(1):161-73.
Magerlein JM, & Martin JB, Surgical Demand Scheduling: A Review. Health Services Research Winter 1998; 13:418-33.
McQuarrie DG, Limits to Efficient Operating Room Scheduling. Archives of Surgery August 1981; 116:1065-71.
Meikle SM, Local area network: Preparing for installation in the operating room. AORN J October 1993; 58(4): 708-13.
Ozkarahan I, Allocation of Surgical Procedures to Operating Rooms. Journal of Medical Systems August 1995; 19(4):333-52.
Przasnyski ZH, Operating room scheduling: A literature review. AORN J 1986; 44(1):
Tan JK: Health Management Information Systems Theories, Methods, and Applications. Aspen, 1995.
Westbrook ML, Dunn SE, & Wilcox-Riggs S, Development of a Comprehensive Surgical Information System at Madigan Army Medical Center. March 1996; 161(3):154-8.
Williams PW, Implementing an informatics system in a perioperative environment. AORN J January 1997; 65(1): 94-7.
Wright IH, Kooperberg C, Bonar, BA, & Bashein, G, Statistical Modeling to Predict Elective Surgery Time. Anesthesiology December 1996; 85(6):1235
Marketing Literature, Internet Web Sites, & Personal Contacts/Interviews for Advanced Medical Systems, Enterprise Systems, Inc., Serving Software Group (HBOC), & Surgical Information Systems.
Advanced Medical Systems' ConTrol system organizes and integrates the entire supply function. All activity, from purchase requisitioning through patient expensing, is brought together, with transactions instantly and simultaneously reflected throughout the system. ConTrol was designed and developed in a multi-entity hospital and continues to excel in multi-facility functionality to monitor the movement of inventory from one hospital to departments or cost centers in other hospitals.
The ConTrol Operating Room module provides the functionality to accurately maintain a surgical case schedule. Operating Room personnel have the capability to modify, record, and monitor all relevant surgical case information. ConTrol provides the means to avoid scheduling conflicts to allow for the efficient management of resources.
The four essential tasks of the Operating Room module include:
The ConTrol Operating Room module also provides accurate item utilization data. Preference Cards and Case Carts enable staff to determine what materials were utilized during the case. This information can then be electronically filed so that the patients can be charged for supplies used and inventory can be replenished and requisitioned, as needed.
The ConTrol Operating Room module is one of several available modules which, as an aggregate, function as an integrated information system. Materials Management, Accounts Payable, Asset Management, Budget Management, and Electronic Data Interchange (EDI) comprise the other available modules.
Enterprise Systems, Inc. (ESi) provides an integrated system, consisting of modules for Surgical Services Management, Materials Management, Accounts Payable, Enterprise Scheduling, and Resource Management.
ESi's ORBIT Surgical Services Management module is rich in functionality to provide for the appropriate utilization of operating room resources.
Physician office staff have the ability to schedule requests on-line remotely. Available, conflict-free booking slots are identified and displayed to the user in real-time. The time needed for the procedure is identified, based on the surgeon's historical performance. A confirmation is sent to the surgeon when the process is completed. Detailed security levels assure that access is limited to the scheduling function.
ORBIT processes inventory for multiple locations and forecasts supply needs. Order quantities are recommended and wasted supplies are tracked
Scheduling patient procedures is completed through a graphical interface. Conflict of resources is checked after the procedure is scheduled. Supplies needed for the case are identified and the time needed for the case is predicted, based on physician preferences and previous performance data.
ORBIT incorporates clinical guidelines for procedure care. A preference list value and surgeon/procedure comparison is identified and then a pick ticket is generated that organizes the supply list by bin location.
A visual display of room setup, instruments, and trays is available in ORBIT.
Multiple procedures are captured which allows for statistical analysis by case and/or procedure. An implant log is used to record trackable devices for the Standard Medical Device Act (SMDA).
Up-to-the-minute case status is used to improve communication and better accommodate emergencies or cancellations to the schedule. Early completions or delays are recorded.
Case cost and expected revenue are compared through report generation. Infection control and QA reports are also available. Staff, surgeon, and anesthesiologist reports aid in documenting regulatory compliance and risk management reporting. Three are over 100 standard reports, available in graphical and chart format. Statistics are available immediately and trends are identified.
SIS computer applications enable a surgical department to accurately schedule procedures, fully document the intraoperative and postoperative episode, and enable the department manager to accurately assess cost components and cost tracking for the totality of the surgical procedure. In addition, SIS provides an added value through surgical pathways and clinical outcome evaluations. The SIS system captures all clinical, financial, administrative, and archival data needed to manage surgical services and comply with JCAHO quality monitoring requirements.
|
Clinical
q Patient Trackingq Clinical Pathwaysq Point-of-Care Documentationq Real-Time Patient Monitoringq Charting by Exceptionq Prompts for Critical Informationq Automated Nursing and Anesthesia Documentationq Outcomes Monitoring and Utilizationq Network-Accessible to all Caregivers |
Administrative
q Schedulingq Efficiency Analysisq Patient Trackingq Preference Cards Management and Utilizationq Materials Managementq Resource Utilization Patternsq Unified Patient Record, Continuously Accessible for Caregiver Updatesq Nursing Classificationq Joint Commission Review Preparation
|
|
Financial
q Labor Costsq Materials Costsq Equipment Cost Allocationsq Overhead Cost Allocationsq Pathway Variance Costsq Billing and Charge Dataq Profit Margin Analysis
|
Archival
q Comprehensive Data Warehousingq Benchmark Researchq Protocol Variance Researchq Retrospective Studiesq Individual Case Reviewq Surgical Quality Assuranceq Payor Negotiation Dataq Case Mixq Payor Mix
|
SIS is based using a Graphical User Interface (GUI) format in which the user can point, click, drop, & drag the cases into the respective slots. Block scheduling accommodates specialty block definition, practice block definition, and surgeon block definition. The SIS system incorporates prep times, clean-up times, and rolling average times for a specified surgeon and a specified case.
When cases are canceled or re-scheduled, resources associated with that particular case are immediately released and cancellation and reschedule patterns can be monitored. Information is archived in a single digital patient record enabling all case information, including case cost and profit margin, to be reproduced immediately upon PACU discharge or at any time thereafter. Each patient record is compiled into a permanent database that is accessed for billing information and retrospective research, among other needs.
The results of the patient interverview process are verified and released to other providers throughout the hospital, not just those using SIS. The patient's physical and history record and baseline for the anesthesia provider to establish the anesthesia administration plan are summarized.
Some of the information that can be recorded by SIS includes: patient history, medication names, handicaps, patient valuables, and a recall feature for patients who have had previous procedures. The preoperative data is stored in a read only format for anesthesia and intraoperative care providers to review.
SIS can simultaneously monitor up to 125 vital signs from as many as 25 patient monitoring platforms. Non-physiological data including the administration of drugs, anesthetic events, patient demographics, event timing, and involved staff is recorded quickly and easily using a GUI. Voice response, touch screens, light pens, or bar coding are available for SIS users.
Information about all equipment, supplies, drugs, and personnel used for a case is tracked and recorded with a date and time stamp. There is a preference card system and a QA module for tracking QA studies. Clinical pathways allow the users to research data for pathways, construct the most cost-effective pathway for the hospital, and monitor pathway variances. SIS records and stores all costs for materials, staff, and equipment, dates and time stamps all activities, gives the user patient demographic information.
SIS has an interface that can monitor a patient's condition during the initial postoperative period and multiple patients can be monitored simultaneously. Routine and other observation information can be entered into the system for a complete medical record. Medications and supplies can also be entered so those items that are to be charged are accurately recorded and available immediately after the procedure has been completed.
A real-time view of the patient's total recovery process, including nursing notes, observations, and comments is displayed. All drugs and fluids administered, recovery scores, pain scores, and vital signs are also recorded and displayed. A recovery nurse Post Anesthesia Care Unit or Recovery Record is created, which is an integral part of the surgical patient's medical record. All costs, personnel, and materials used for a case are captured in the patient medical record.
HBO's Serving Software Group's Surge-Server is the leading operating room scheduling and management system. Surge-Server manages case scheduling, charging, charting, staff scheduling, and reporting.
Each Surge-Server system is personalized, allowing users to define screens, data elements, screen flow, abbreviations, and data flow.
The Surge-Server Surgical Scheduling module is flexible and can be complemented by the addition of the following modules: Dynamic Scheduling, IntraOperative, Multi-Entity, Surgical Personnel, and Surgical Supply. An Accounts Payable module, however, is not available as a component of an integrated system, although other vendor's products can be interfaced to Surgi-Server.
The Surgi-Server system streamlines patient scheduling, optimizes resource management, simplifies data analysis, and maximizes operating room utilization. Surgi-Server effectively assists in the management of all surgery resources, including room, equipment, supplies, and personnel.
A variety of scheduling techniques optimizes scheduling decisions. The system improves scheduling accuracy and efficiency through the use of speed scheduling and wait-lists. Speed scheduling allows users to search for conflict-free case starting times for a specific date and time range. The wait-list capability allows users to collect patient and case information without confirming a scheduled time.
Surgi-Server produces a printed pick-list, to notify the central supply department in advance of the necessary supplies required for scheduled cases. Pick-lists are important tools for improving charging accuracy and dramatically reduce the incidence of lost charges, while providing valuable procedure cost information.
Surgi-Server is designed to be intuitive, requiring users to have only minimal computer knowledge, with most functions accessed by point-and-click technique.
A library of standard reports provides extensive data on volume, utilization, cancellations, and delays; user-defined reporting allows users to create reports on an ad hoc basis.
Go back to the Project Page
Rema Padman, rpadman@andrew.cmu.edu